

Arthritis (Osteoarthritis) and Physiotherapy
Arthritis (Osteoarthritis) and Physiotherapy
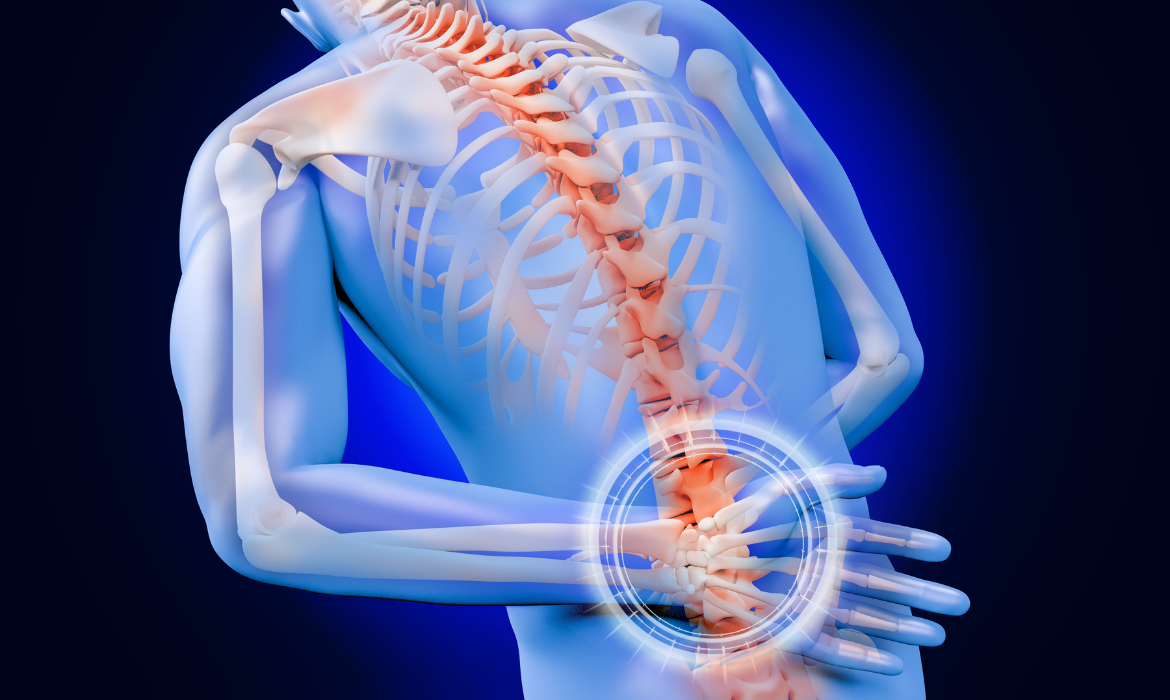
Osteoarthritis is basically wear and tear or age related degeneration of the cartilage that lines the bony surfaces of a joint and potentially the bone itself, such as the hip/knee/spine/shoulder/thumb and other finger joints. Any joint can get arthritis, but these are the most common joints to be affected by arthritis.
Some people get earlier and more severe arthritic changes in one or more joints. This may be secondary to a previous injury or joint fracture, or due to unbalanced/uneven alignment of the joint surfaces such as with knock knees, bowed legs at the knees, hip dysplasia/leg perthes disease/clicking hip from birth, scoliosis of the spine etc. Arthritic/degenerative/normal wear and tear changes to our joints does not necessarily mean someone will be in pain. Many people have arthritis and do not experience pain or deterioration in their function. It more depends on the severity of the degeneration and many other factors. Some people have very minor degeneration but may experience significant pain. Others have similar or worse degenerative changes and do not experience pain. A very important rule or recommendation all therapists/doctors need to keep in mind is- TREAT THE INDIVIDUAL, NOT THE MRI/X-RAY. Of course, MRI/X-ray/other imaging results can be very informative and helpful in guiding assessment and treatment, especially in ruling out more serious pathology where there is any suspicion of this based on symptoms/previous history.
Joint cartilage when worn down will lead to increased stress on the bone surface underneath and if the wear is uneven it can lead to increased stress on parts of the joint surfaces that are experiencing more compression and weight bearing or load than the surfaces that are less compressed and loaded. This is similar with an engine or machine that is out of alignment, you will get more wear and tear on the surfaces that are experiencing more compression under load. That is why realignment/tune-ups/services of engines/machines prolong the life/good functioning of the engine/machine. Similarly, appropriate and effective PHYSIOTHERAPY can really facilitate the optimum functioning of your joints, thus helping to reduce pain and wear and tear/degeneration of the joints of the leg/arm/spine/pelvis and improve function and quality of life.
SO HOW CAN APPROPRIATE/EFFECTIVE PHYSIOTHERAPY HELP WITH ARTHRITIS?
- Improving/optimising JOINT ALIGNMENT
- Improving/optimising muscle/joint/ligament/tendon PLIABILITY/FLEXIBILITY (basically all the soft tissue/connective tissues of the local symptomatic joint system and any and all of the joint/muscle/ligament/tendon/neurovascular/viscera or organ structures that may impact on the symptomatic joint.
- Improving/optimising STRENGTH of the local/primary muscles working on the involved joint and muscle strength of all muscles that can impact on the effective/efficient function of the involved joint. So if a person has degenerative changes of the tendons/muscles of the rotator cuff that control shoulder joint movement it is important to strengthen/enhance loading ability of these rotator cuff muscles and tendons to attain pain free function of the shoulder, but strength of the leg muscles is a very important factor in shoulder function, as is strength of the core muscles of the core/abdomen/spine. Likewise, for the knee, strength of the prime movers of the knee is very important, but strength of the hip muscles is crucial to the function of the knee. The stronger all of the associated muscles are, the less stress is placed on the involved joint.
- Also, for the knee joint, for example, the alignment of the ankle and foot joints can be very important. So for example, if the foot is flat or pronated, this may have an affect on the knee joint, potentially causing compression and more stress on the outside or lateral compartment of the knee joint, possibly being a contributing factor to wear and tear of the outside/lateral compartment of the knee joint. If the foot is supinated, or the opposite to flat foot, this can cause increased stress on the inside or medial compartment of the knee joint. Addressing alignment of the ankle and foot joints and associated muscle/ligament/tendon flexibility/function can have a positive effect on the alignment/function of the knee joint. Orthotics/insoles potentially may a have role in and be of benefit in optimising the foot/ankle alignment, thus impacting the alignment/function of the knee joint. This can also affect the hip joint and the spine. Physiotherapists if trained in this biomechanical assessment of the foot/ankle complex can assess if insoles will be of benefit in the management of the knee joint issues/pain/function, and if appropriate can prescribe what is needed in an orthotic/insole to address the biomechanical issues present.
- Cardiovascular fitness and more optimum body weight may also be factors that are pertinent with some people to help optimise joint function. Psychosocial (stress factors) and lifestyle factors (sleep, diet, exercise, work/life balance) may be of relevance to greater or lesser degrees. Effective physiotherapy should help address these factors and refer onto appropriate health professionals as needed.
- A combined approach is called for to address all contributing factors to a person’s symptoms and function.
Back Pain vs. Sciatica: What’s the Difference?
Back pain is the most commonly experienced type of pain. It usually develops from a muscle strain or injury, but sometimes your discomfort may not be just general back pain, it could be sciatica.
Sciatica, while it still falls under the definition of “back pain” is a very specific type. It is also incredibly common. Sciatica is typically felt in the lower back, legs, or buttocks, and it develops from issues surrounding the nerves. Whether you’re experiencing general back pain or sciatica pain, physiotherapy can help relieve your symptoms and restore you to optimum levels of physical function.
In many cases, physiotherapy treatments can even eliminate the need for harmful pain-management drugs, such as opioids, or an invasive surgical procedure.
Why do back pain and sciatica occur?
The most common cause of back pain is from sustaining an injury. This can happen in one of two ways – from an instant, sudden trauma (such as a car accident) or from a repetitive-use injury that develops gradually over time (such as bending down multiple times throughout the week to pick up heavy boxes). Back pain can also result from underlying conditions, such as herniated discs, which can also lead to sciatica. Degenerative disc disease is another common culprit for back pain, which is typically caused by obesity or poor posture. Those who suffer from degenerative disc disease usually report feeling chronic dull aches in their lower back.
The medical term for sciatica is “lumbar radiculopathy,” and unlike general back pain, it is a bit harder to understand. Sciatica typically affects people aged 30-50, and there are several different ways in which it can develop. Certain conditions can lead to sciatica, such as bone spurs, arthritis, or any injury that affects the sciatic nerve. Injuries can also lead to sciatica, such as herniated discs, harsh falls, sports-related collisions, or anything that occurs gradually over time through overuse, repetition, or general “wear and tear.”
Knowing the difference:
Back pain
“Back pain” is an all-encompassing term used to describe a vast number of conditions that cause pain in the upper or lower back. Sports-related injuries, poor posture, and car accidents are just a few of the many ways that someone can develop back pain.
Back pain can be described as either acute or chronic. Acute pain means that it lasts for a short time and is usually severe. Chronic pain means that it lasts generally three months or longer and it can either cause dull or severe persistent pain. The pain you experience is typically either rooted in your back muscles or the bones in your spine.
No matter what the case may be, physiotherapy can formulate a treatment plan based on your specific back pain, its location, and your medical history.
Sciatica
Those who have experienced sciatica typically report it as being very uncomfortable. Fortunately, it is also fairly easy to diagnose.
Sciatica pain is typically reported as being very uncomfortable. People with sciatica suffer from pain along their sciatic nerve, which is the biggest nerve in the human body. The sciatic nerve begins at the lower back, splitting at the base of the spine to extend down the buttocks, both legs, and ends at the bottom of each foot.
Sciatica occurs when the sciatic nerve becomes “pinched” or otherwise damaged in some way, thus resulting in a “stinging,” “burning,” or “shooting” sensation in the lower back, buttocks, legs, or feet.
Physiothaerapy can address a lot of the causes of this compression on the sciatic nerve, thus helping to alleviate the pain

Insoles/Orthotics/Shoe Inserts
Insoles/Orthotics/Shoe Inserts
If appropriate, based on a person’s history/symptoms, a biomechanical assessment will be performed to see if a person may require insoles/orthotics/shoe inserts to help in relieving symptoms and strain on joints/muscles/tendons/ligaments of the lower limb/pelvis/spine, to optimise a person’s function and comfort. This may help with problems such as pain/dysfunction associated with many conditions including:
Flat Feet/Pronated Feet
Supinated Feet
Plantarfasciitis
Hallux Valgus/Bunion
Hammertoes/Corns
Osteoarthritis/Pain in any of the joints of the toes/foot/ankle/knee/hip/spine
Achilles Tendinitis
ITB (iliotibial band strain)
Growing Pains
Appropriate Therapeutic Exercises will be given in conjunction with insoles to help improve the function of the foot/ankle complex/lower extremity strength and flexibility/balance mechanisms as appropriate for an individual.
Many times a person may only require arch support suitable to their arch profile (low/medium/high arch profile -called the longitudinal arch) to help to optimise the alignment and function of their foot and lower limb.
Sometimes in addition some extra support may be required to the rear foot &/or forefoot to achieve better alignment and support. Sometimes a person may need extra support to the arch behind the balls of the toes (transverse arch) to help take increased stress off the balls of the toes (often evidenced by the accumulation of hard skin under the balls of the toes, and possibly corns on the top of the toes).
Sometimes the joint at the base of the big toe may be very stiff (Hallux Rigidus). This can really interfere with walking at the part of gait where you are going up on your toes, at the end foot contact to the floor before that foot comes off the ground to go into the swing phase, causing pain at the base of the big toe and possibly decreasing stride length. Different accommodations to the insole can help this problem. Sometimes adding more support behind the balls of the toes to the transverse arch helps, or incorporating a cut out under the joint creating a small depression allows for more pain-free movement here. Sometimes more support is required under this joint to decrease movement and stress at this joint.
Occasionally a heel lift may be required to take strain off of an achilles tendinitis during the initial healing phase, or if there is a true leg length difference to help equalise leg length. I find this is quite rare. Often there can be an apparent leg length difference, as a consequence of a twist or rotation of the pelvic bone on one side. If a pelvic bone is twisted forwards on one side, it can make that leg appear to be longer than the opposite leg. If a pelvic bone is twisted backwards on one side, it can make that leg appear to be shorter than the other leg. When there appears to be a leg length difference I would always assess for a twist of the pelvis and if present treat that and then reassess leg length. Then if there is still a leg length difference present this can be accommodated for with an appropriate heel raise, but again I rarely find this to be the case.
I aim for the least bulky corrections needed to help maximise comfort and compliance in using/wearing any accommodative inserts/insoles. I also aim for the least costly but effective inserts/insoles. Sometimes just more supportive/appropriate shoe-wear is all that is required. Frequently off the shelf devices are totally appropriate and these are very reasonably priced. There is a huge range of good off the shelf devices/insoles available from orthotic companies that suit different situations. Sometimes a customised insole is required where a cast is made and along with the biomechanical assessment the appropriate insole is prescribed and ordered from on orthotic company. I always aim to keep the solution where required effective and at a very cost-efficient fee, not adding any profit margin, just covering my cost. The orthotic companies I deal with also offer a big range of shoe-wear that suits an individual’s foot and their activities, and these can be ordered and again I pass on the cost that I pay for them.

Recent Comments